
Introduction
In March 2020, the World Health Organization officially recognized COVID-19 as a global pandemic (WHO, 2020), which prompted governments worldwide to introduce extensive public health measures aimed at limiting virus transmission (Amd et al., 2024). In Poland, this resulted in the declaration of an epidemic emergency and the enforcement of nationwide lockdown measures. These restrictions included limits on gatherings exceeding 50 individuals, closure of cultural venues, restaurants, shopping centers, as well as restricted access to religious institutions and fitness facilities (Adamczak et al., 2025). Additionally, schools, universities, and workplaces were required to transition to remote operations (Regulation of the Minister of Health, 2020), which significantly disrupted daily routines. It was not until May 2022 that the Polish Minister of Health officially lifted the state of the epidemic, marking the formal end of the pandemic in the country (Augustynowicz, 2022). For young adults, these sudden and far-reaching changes negatively affected academic progress, social interactions, and everyday habits, requiring rapid adaptation to a more isolated and sedentary lifestyle (O’Reilly et al., 2021). The abrupt loss of structure, reduced face-to-face interactions, and prolonged uncertainty were associated with increased stress, anxiety, and emotional burden, ultimately affecting psychological well-being (Buheji et al., 2020).
Moreover, medical students tend to report higher stress levels than their non-medical peers (Mirza et al., 2021; Wege et al., 2016). Research has consistently shown that this group reports elevated rates of anxiety, depression, and burnout, which are often linked to the demanding nature of medical education and preparation for future professional roles (Shah et al., 2010). In addition to academic stressors, first-year medical students undergo a transition phase involving adaptation to independent living, financial responsibilities, and new social environments (Heinen et al., 2017). The combination of academic and psychosocial stressors may increase the risk of developing maladaptive coping mechanisms.
The role of physical activity (PA) in mitigating stress and enhancing mental well-being has been widely described in the literature (Herbert, 2022). Regular PA is associated with reduced levels of anxiety, improved mood, and better cognitive function (Mandolesi et al., 2018). However, studies indicate that medical students often engage in insufficient levels of PA due to time constraints, academic workload, and declining motivation (Taylor et al., 2022). The COVID-19 pandemic further exacerbated this issue, as lockdown measures resulted in the closure of gyms and recreational spaces, limiting opportunities for exercise and increasing sedentary behavior (Ullah et al., 2021). Multiple studies have examined the association between pandemic-related conditions and medical students' well-being, revealing significant increases in stress, anxiety, and depressive symptoms (Alkureishi et al., 2022; Kosendiak, Wysocki et al., 2023a). A growing body of literature suggests that in the post-pandemic period, levels of PA and psychological well-being have not fully returned to pre-pandemic patterns (Bertocchi et al., 2021; Líška et al., 2024; Woon Teen et al., 2024). Female students, in particular, have been shown to report higher levels of stress and emotional distress than their male counterparts (Ragab et al., 2021). Additionally, there is evidence suggesting that physically inactive individuals experience greater psychological distress, reinforcing the bidirectional relationship between PA and mental health (Denche-Zamorano et al., 2022).
First-year medical students were selected as the focus of this study due to their inherently high baseline stress levels and the distinct challenges they encounter in the early stages of their medical education, compounded by psychosocial stressors (Jordan et al., 2020). These challenges were further intensified by the pandemic, with additional stressors such as disruptions to educational activities, limited opportunities for practical training, and concerns regarding their own health and that of their families (Carletto et al., 2024). Moreover, as future healthcare professionals, medical students will play a pivotal role in addressing public health crises, highlighting the importance of understanding and addressing factors that influence their mental and physical well-being (Grace, VanHeuvelen, 2019; Lewis, Zauskova, 2021).
This study, conducted in June 2022 following the official end of the epidemic in Poland, aimed to assess PA levels and perceived stress levels among first-year medical students during the post-pandemic period and to analyze the association between these variables. The study also aimed to compare these variables and their associations between female and male students to better understand potential gender-related differences in this population.
The findings of this study may provide valuable insights for developing strategies to support medical students and enhance their resilience in the face of future healthcare challenges.
Materials and Methods
Design of the study
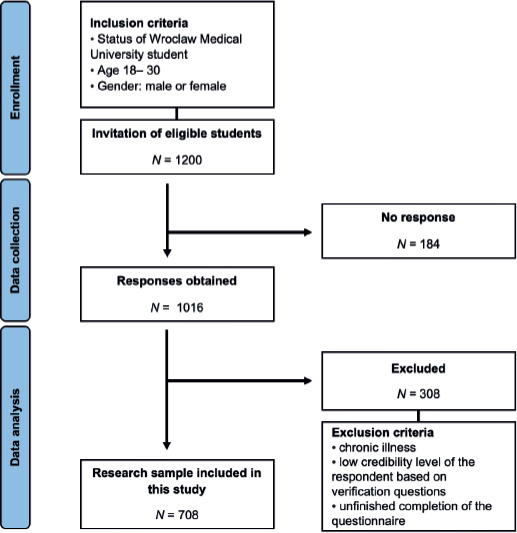
This study adopted a cross-sectional design and included first-year students at Wroclaw Medical University, a leading public medical school in Wroclaw, the fourth-largest city in Poland, in the western part of the country. The university enrolls approximately 6,000 students, including over 900 international students, creating a diverse and vibrant student community. The primary aim of this study was to assess baseline stress levels and examine the association between perceived stress and PA among medical students in the post-pandemic period. Data were collected in June 2022. During this time, students enrolled in mandatory PE classes were invited to participate in anonymous online surveys, distributed through dedicated links. A total of 1200 students were invited to participate in the study, of whom 708 provided complete questionnaires included in the final analysis, resulting in a response rate of 59%. The study included students attending mandatory physical education classes during the first year of medical studies. Incomplete questionnaires and responses identified as unreliable due to logical inconsistencies or substantial missing data were excluded from the final analysis. No additional weighting or imputation procedures were applied to missing data. All students meeting the eligibility criteria were encouraged to participate, aiming to capture a broad spectrum of experience within the cohort. Participants received detailed information regarding the purpose of the research; their involvement was entirely voluntary and based on informed consent procedures. A comprehensive overview of the data collection procedures, as well as the inclusion and exclusion criteria applied, is provided in Figure 1. Participants with chronic illnesses were excluded because their typical PA behaviors may significantly differ from the norm, and the group size was too small to allow for meaningful statistical analysis in this regard. This exclusion limits the generalizability of findings to clinically healthy students’ populations only.
Statistical Analysis
Data cleansing and computation were performed using Microsoft Excel (version 16.77, Redmond, WA, USA), and all statistical analyses were carried out using Statistica 13 software (Statsoft, Kraków, Poland). P-values < 0.05 have been deemed statistically significant.
Descriptive statistics included frequency and percentage calculations for categorical data; and the mean, median, and interquartile range (IQR) for continuous variables. The Shapiro-Wilk test indicated non-normal data distribution; therefore, non-parametric tests were applied. Comparisons between two independent groups (female vs. male students) were performed using the Mann-Whitney U test, while comparisons involving more than two groups were conducted using the Kruskal-Wallis test followed by post hoc multiple comparison procedures. To reduce the risk of type I error associated with multiple comparisons, post hoc analyses were adjusted using the Dunn-Bonferroni correction. Effect sizes were additionally considered for interpretation of group differences (where applicable). Additionally, Spearman’s rank correlation coefficients were calculated to assess associations between continuous PA and perceived stress variables.
The k-means clustering method was applied, utilizing Euclidean distance as the measure of distance between observations. Prior to clustering, all variables included in the model were standardized (z-scores) due to differences in measurement scales between MET-min/week variables and stress questionnaire scores. Standardization was essential to prevent variables with larger numerical ranges from disproportionately influencing clustering results. The optimal number of clusters was selected based on v-fold cross-validation and interpretability of the obtained cluster profiles. Cluster stability was additionally verified through repeated iterations of the algorithm using different initial centroid positions. However, no external validation dataset was available, which should be considered when interpreting cluster robustness. The following variables were used in the model: Walking MET-m/w, Moderate MET-m/w, Vigorous MET-m/w, ET, ES, IS, LS, OS (Kosendiak et al., 2025).
International Physical Activity Questionnaire (IPAQ)
The PA levels were evaluated using the IPAQ, a self-reported questionnaire that captures PA behaviors. The IPAQ has been widely validated and shown to be a reliable tool in numerous studies, including those conducted in Polish populations (Adamczak et al., 2023; Bergier et al., 2012; Craig et al., 2003). It includes seven items: six questions focus on the frequency and duration of walking, moderate-intensity, and vigorous-intensity activities over the past seven days, while the seventh question assesses the amount of daily sitting time. To minimize potential overreporting, participants were provided with detailed instructions prior to completing the questionnaire (Biernat et al., 2007).
PA data were calculated by multiplying the duration of each activity by its corresponding metabolic equivalent (MET) value: walking (3.3 MET), moderate-intensity activity (4.0 MET), and vigorous-intensity activity (8.0 MET). The resulting values were expressed as MET-minutes per week (MET-m/w) (Hagströmer et al., 2006).
The Perception of Stress Questionnaire (KPS)
To determine the perceived psychological stress levels among participants, a twenty-seven-item psychological tool – the KPS (Plopa, Makarowski, 2010) – was used. The validity and reliability of the KPS have been established through prior studies, including those conducted within Polish samples (Kosendiak et al., 2022; Plopa, Makarowski, 2010).
All items in the questionnaire were assessed using a five-point Likert scale, ranging from “true” to “not true”. This questionnaire evaluates several dimensions of perceived stress, including: Internal Stress (IS) – characterized by inner turmoil, worry, and self-doubt; External Stress (ES) – refers to stress arising from external pressures or demands, often associated with feelings of being treated unjustly; Emotional Tension (ET) – measures feelings of irritability, anxiety, and restlessness; Overall Stress (OS) – combines the scores of IS, ET, and ES; Lie Scale (LS) – used to identify a tendency to present oneself in an overly favorable manner. Results are reported on a Standard Ten Scale, prepared to account for different socio-demographic profiles.
Results
Table 1 presents the general characteristics of the study participants. The majority of the study group were women (80.8%). Most participants resided in urban areas, with nearly half living in the largest cities. Approximately three-quarters of the participants had a normal BMI, with a similar number of individuals having either a too-high or too-low BMI, around 12%.
Table 1
Characteristics of study participants
Table 2 displays the level of PA, categorized by gender. Just over 20% of individuals in both genders met the Health-Enhancing PA (HEPA) criteria. A lower proportion of men were classified as inactive. Most participants were minimally active, with this group comprising between 60% and 70% in both genders.
Table 2
PA levels
| PA level | N (%) |
|---|---|
| Females | |
| Inactive | 82 (14.3) |
| Minimally active | 371 (64.9) |
| HEPA | 119 (20.8) |
| Males | |
| Inactive | 9 (6.6) |
| Minimally active | 95 (69.9) |
| HEPA | 32 (23.5) |
Table 3 compares the study variables between genders. The primary component of PA for both genders was walking. There was no significant difference in Moderate and Walking PA. Men had higher levels of Vigorous PA, though this did not affect Total PA levels. Regarding stress levels, the only domain without a significant difference between genders was ES, with all other domains showing higher levels in females.
Table 3
Study variable differences between genders
Table 4 outlines the differences in stress levels based on PA levels. Among women, those meeting the HEPA criteria had lower perceived stress levels compared to less active individuals in the ET, ES, IS, and OS variables. For men, none of these relationships were statistically significant.
Table 4
Differences between stress domains and PA levels in genders
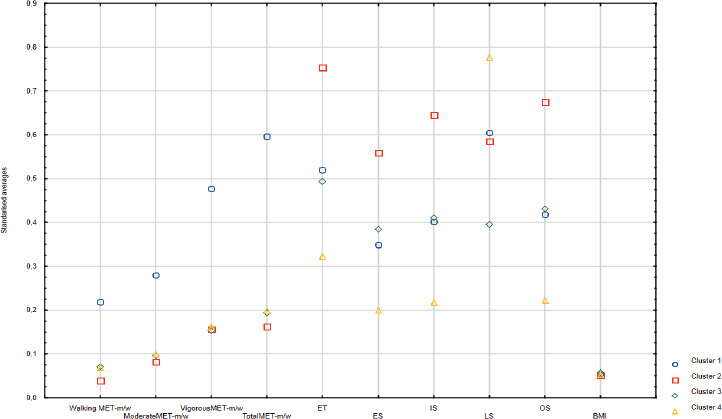
Table 5 presents a comparison of the variables among the clusters obtained from the cluster analysis. Cluster 1 is characterized by the highest values in all PA levels and relatively low stress levels. Cluster 2 exhibits low PA levels, the highest stress levels, and a moderate LS score. Cluster 3 is defined by low PA, moderate stress levels, and a high LS score. Finally, Cluster 4 is characterized by moderate PA, the lowest stress levels, and the highest LS score. These variables are also presented graphically in Figure 2.
Table 5
Cluster analysis
Discussion
The present study aimed to examine the relationship between PA and stress levels among medical students in the post-pandemic period. The findings provide important insights into behavioral patterns in this population and partially support the assumption that higher levels of PA are associated with lower perceived stress.
Anthropometric Data
This study examined PA, perceived stress, and their association among students at Wroclaw Medical University during the post-pandemic period. The research cohort predominantly comprised women, reflecting the higher proportion of female students typically enrolled in medical universities (Moberly, 2018).
BMI analysis indicated that approximately 12% of participants were underweight (BMI < 18.5) and 12% were overweight or obese (BMI ≥ 25), with nearly one-quarter presenting abnormal BMI values. These findings are consistent with a longitudinal study of Polish nursing students from 2019 to 2021 (23.44% abnormal BMI on average) (Kosendiak, Wysocki et al., 2023b) and a recent study on Polish medical students (Kosendiak, Adamczak et al., 2023). Compared to other populations, such as those in Poland (36.3%) (Sidor, Rzymski, 2020) and Spain (30.3%) (Sumalla-Cano et al., 2022), our results are more favorable in terms of lower abnormal BMI rates. This may suggest relatively better weight-related health behaviors in the studied cohort, although this interpretation should be approached with caution due to methodological constraints. It is important to acknowledge, that BMI's limitations as a measure of body fat should be noted, as it does not distinguish between fat and muscle mass, potentially misclassifying athletic individuals as above the normal weight range (Burkhauser, Cawley, 2008).
Physical Activity
The pandemic significantly affected PA through various public health restrictions, contributing to increased sedentary behavior (Sekulic et al., 2022). Remote and asynchronous physical education classes may have further reduced motivation and access to equipment, leading to decreased PA levels (Wijngaards et al., 2022). Extensive research indicates a decline in walking, moderate, vigorous, and overall PA levels among university students across various countries during periods of confinement imposed by the COVID-19 pandemic (Ferrara et al., 2022; López-Valenciano et al., 2020; Roggio et al., 2021). This study aimed to investigate whether these negative PA habits persisted in the post-pandemic period.
The research assessed various PA types among medical students, revealing that walking contributed the largest proportion of total MET-m/w for both genders, accounting for 71.8% amongst women and 64.6% amongst men and 50.7% of total activity. This is a higher score compared to other studies, which documented a declining trend in the percentage of walking MET-m/w relative to total activity during the pandemic, decreasing from 40.7% to 24.2% of the total PA time (Sekulic et al., 2022). The prevalence of walking post-pandemic can be attributed to its accessibility, low cost, and ease of incorporation into daily routines, as well as habits formed during the pandemic. These findings indicate a dominance of low-intensity PA, which may not be sufficient to meet recommended guidelines and, consequently, may not confer the anticipated health benefits. This suggests that although overall activity levels may appear satisfactory, their qualitative structure may limit potential health benefits, which is particularly relevant in the context of preventive health behaviors among future healthcare professionals. Previous studies suggest that even short durations of vigorous PA (e.g., 15-20 minutes per week) may be associated with a reduced risk of cardiovascular mortality (Ahmadi et al., 2022). Thus, it highlights the significance of raising awareness regarding the health advantages associated with vigorous PA.
Our findings indicated relatively high levels of vigorous activity for both genders, with mean MET scores of 596.8 m/w for women and 795.5 m/w for men. This contrasts with longitudinal studies conducted during the pandemic, such as those on Italian adults (267.15 MET-m/w at the beginning, lowered to 143.17 MET-m/w) (Franco et al., 2021) and American adults (335 to 276.39 MET-m/w) (Yang, Koenigstorfer, 2020). This increase may reflect a rebound effect following the lifting of pandemic-related restrictions, suggesting a partial recovery of more intensive forms of PA. Additionally, the higher vigorous MET-m/w scores among men compared to women were statistically significant. This observation is in line with findings reported in previous studies showing that male students tend to have higher levels of Vigorous MET (Trost et al., 2002). Large-scale analyses involving adolescents have shown that boys consistently engaged in greater levels of moderate-to-vigorous PA than girls, with the disparity being most pronounced among older adolescents (Araujo et al., 2024). Likewise, a 2022 study conducted in Ireland highlighted higher MET-m/w among males compared to their female counterparts (McCarthy, Warne, 2022). Further corroboration comes from a Spanish study involving more than 3,000 university students, which indicated that males participated in substantially higher levels of moderate-to-vigorous PA than females (Espada et al., 2023). However, the median vigorous MET-m/w value of 596.8 for women in this study was more favorable compared to the median of 0 reported in a similar cohort during the pandemic (March 2021), where most women were not engaged in such exercises. Additionally, the observed general increase in vigorous PA levels may be attributed to the reopening of gyms and sports facilities following the pandemic.
The study also assessed 12.8% of the students as inactive, a significant improvement compared to the 80.7% inactivity rate in a comparable 2021 cohort (Kosendiak, Adamczak, et al., 2023). However, this rate remains higher than the 4.6% inactivity observed in middle-aged Brazilians during the pandemic (Puccinelli et al., 2021). Conversely, 87.2% of students in our study were physically active, a much higher rate than the 49.5% found in a pre-pandemic 2015 study of Thai medical students (Wattanapisit et al., 2016). Furthermore, slightly more than 20% of students achieved HEPA levels, which is slightly higher than the average 11% reported in a Polish longitudinal study conducted during the pandemic, in October 2020 and March 2021 (Kosendiak, Adamczak, et al., 2023), but significantly lower than the 61% adherence to health-related PA recommendations observed in U.S. medical students pre-pandemic (Frank et al., 2008). Despite improvements in vigorous MET-m/w scores and lower inactivity rates compared to pandemic-era cohorts, the low percentage of students achieving HEPA levels remains concerning. Overall, these findings indicate that although certain aspects of PA improved in the post-pandemic period, achieving recommended activity levels remains a challenge in this population. These findings underscore the need to promote awareness of the importance of sufficient PA intensity among medical students.
Stress Levels
In four out of five tested variables concerning stress levels, female medical students demonstrated significantly higher scores than males, particularly in overall scores in stress levels, perceived emotional tension, and intrapsychic stress. A longitudinal study conducted in Poland reported reduced anxiety levels among medical students in the post-pandemic period. Moreover, the study found that female students experienced higher stress levels than their male counterparts in both 2020 and 2022, a finding consistent with our results (Wróblewski et al., 2024). These higher scores among women align with existing research (Ishiguro et al., 2019; Vigna et al., 2019). Other studies conducted during the COVID-19 pandemic also found that females experienced greater stress than males (Xiong et al., 2020; Yan et al., 2021). Gender differences in stress are associated with social, psychological (Slavich, Sacher, 2019), cognitive processes, and biological factors, including hormonal fluctuations (Albert et al., 2015; Goldstein et al., 2010). These mechanisms may help explain the consistently higher stress levels observed among female students in both the present and previous studies.
Previous research on student populations has also shown that women score higher on the Lie scale compared to men (Al-Turkait Ohaeri, 2016; Molinuevo, Torrubia, 2013). It has been reported that higher scores on the Lie scale are associated with neuroticism (Hart et al., 2020). Compared to individuals with low neuroticism, those with high neuroticism report more interpersonal stressors, employ less adaptive coping strategies (e.g., hostile reactions), and exhibit greater distress (Gunthert et al., 1999). Therefore, the disparities in perceived stress levels between genders in our study are further corroborated by higher scores on the lie scale among women. These differences underscore the greater need for psychological support services especially among females, necessitating targeted governmental interventions to enhance resilience and reduce distress.
Furthermore, the median levels of ES and scores on the LS were higher among women in our study cohort compared to the general population. This finding is consistent with research involving over 40,000 medical students, which stated the global prevalence among medical students to be 33.8% (Tian-Ci Quek et al., 2019), while the prevalence of anxiety in the general population is estimated to be 3% (Henry, Crawford, 2005). This discrepancy is likely because medical education is considered one of the most academically and emotionally demanding training programs across all professions (Dyrbye, Shanafelt, 2016). Additionally, there is a high prevalence of neuroticism among medical students, with female students exhibiting higher rates than male students, which predisposes them to elevated stress levels (Tyssen et al., 2007).
Relationship between Physical Activity and Stress Levels
Our study identified a statistically significant relationship between PA and perceived stress levels among female students. Previous studies have suggested that PA may be associated with biological and psychological mechanisms linked to stress regulation; however, these mechanisms were not directly assessed in the present study (Wright et al., 2005). Therefore, our results align with the broader scientific consensus that HEPA is associated with lower perceived stress. Further supporting this, studies on medical students have reported similar conclusions (Tung et al., 2020). A pre-pandemic Polish study revealed that medical students with higher levels of PA exhibited lower stress levels (Dąbrowska-Galas, Dąbrowska, 2022). Additionally, an American study of a similar cohort found that medical students who achieved HEPA were 26% more likely to be in the lowest stress quartile and 22% less likely to be in the highest stress quartile (Leuchter et al., 2022). Given that our study found women to have lower levels of PA and greater perceived stress compared to men, alongside very low HEPA levels in both genders, it is imperative to tailor future educational efforts, especially towards women, emphasizing the positive impact of PA on stress reduction.
Our study did not reveal a statistically significant relationship between PA and stress levels among male students. Contrarily, an American study on students demonstrated that PA was more strongly correlated with perceived stress in males than in females (Peyer et al., 2024). Another study found that male students exhibited significantly greater initial reductions in anxiety compared to females following one week of exercise, although these gender differences were no longer apparent after two weeks (Medina et al., 2014). Additionally, a study conducted in 2012 revealed gender-specific differences in the mental health benefits of PA, with men deriving more significant advantages from vigorous PA, whereas women experienced greater mental health improvements from engaging in moderate PA (Asztalos et al., 2012). These findings underscore the need for further research to elucidate gender differences in the effects of PA on stress levels.
The comparison of the variables among the clusters identified through cluster analysis revealed distinct patterns in PA levels and stress scores. Cluster 1 was characterized by the highest levels across all PA categories and relatively low stress levels, which aligns with our aforementioned findings and existing literature suggesting a negative correlation between PA and stress (Andrade et al., 2020). In contrast, Cluster 2 showed low PA levels and the highest stress levels. These results further support the well-documented inverse relationship between PA and stress. Additionally, Clusters 3 and 4 displayed more complex profiles, with Cluster 3 showing low PA and moderate stress levels, while Cluster 4 exhibited moderate PA levels and the lowest stress scores. Interestingly, both clusters also had the highest LS scores, which may suggest a tendency toward underreporting or socially desirable responding. This discrepancy with the existing research should be interpreted cautiously due to the elevated LS scores observed in these clusters, which may reflect socially desirable responding (Grimm, 2010) or other factors influencing self-reporting (Mondal, Mondal, 2018).
Overall, the findings of this study suggest that PA may be associated with stress regulation among medical students, however, this relationship appears to be influenced by gender and potentially other psychosocial factors. This highlights the need for more individualized approaches when designing interventions aimed at improving both mental health and PA levels in this population.
Future Implications
The findings of our study underscore the need for tailored educational interventions and programs addressing the distinct needs of male and female medical students in PA and stress management, especially in the post-pandemic period. Female students exhibited higher stress levels and lower PA levels, highlighting the importance of promoting PA among women. Initiatives should emphasize PA’s mental health benefits through targeted campaigns, workshops, and seminars. Given the very low HEPA levels in both genders, informational campaigns should focus on PA guidelines and the long-term health benefits of achieving HEPA standards. Furthermore, there is a significant need for additional research to examine the current, fully post-pandemic state of students’ PA and stress levels. By implementing gender-specific educational interventions and leveraging post-pandemic insights, universities can foster a supportive environment that promotes regular PA and reduces stress, improving students’ well-being and equipping them with healthy lifestyle habits for their future. These findings also highlight the importance of integrating PA and mental health promotion into medical education.
Limitations
Although this study provides important insights, it is important to acknowledge its inherent limitations. The research cohort, consisting exclusively of students from Wroclaw Medical University, reflects a specific population group, which may limit the generalizability of the findings to the broader population (Kosendiak et al., 2024). This limitation is particularly relevant while interpreting the results in a wider sociocultural context, as both PA patterns and stress perception may vary across different academic environments and populations. Additionally, the predominance of female participants in the cohort may further restrict the applicability of results for the male group. The use of an online survey methodology also introduces the possibility of misinterpretation of questions by participants, despite efforts to provide clear instructions (Adamczak et al., 2025). Moreover, studies based on self-reported questionnaires inherently depend on subjective assessment, which can be subject to bias. This is especially important in the context of the present study, as self-reported measures of both PA and stress may be influenced by recall bias and social desirability, potentially affecting the observed relationships between these variables. Although IPAQ is a widely validated instrument, it may overestimate PA levels compared to objective assessment methods such as accelerometry. To address these limitations, future research will aim to incorporate objective assessments of PA and stress levels in conjunction with questionnaire evaluations, thereby providing a more accurate depiction of the subject matter. Consequently, caution should be exercised when generalizing the observed behavioral characteristics to the larger adult population. It is advisable for future research endeavors to include a more diverse and expansive participant pool to enhance the applicability and depth of the findings presented in this study (Kosendiak et al., 2024). Due to the cross-sectional design, causal relationships between PA and perceived stress cannot be established. Future studies should also explore additional factors that may influence the relationship between PA and stress, including psychological, environmental, and educational determinants.
Conclusions
This study examined the relationship between PA and stress levels among medical students at Wroclaw Medical University in the post-pandemic period. The findings reveal notable gender differences and highlight differences in PA and perceived stress levels among medical students assessed during the post-pandemic period.
Female students exhibited greater perceived stress and lower PA compared to their male counterparts. This aligns with previous research showing greater stress among women, potentially due to physiological and cognitive differences. The higher stress levels in females, coupled with lower PA, underscore the need for targeted interventions to promote PA as a stress reduction strategy, particularly among female students.
The findings suggest that some PA patterns observed during the post-pandemic period may differ from those reported in earlier pandemic-related studies. Our study also revealed that, despite a general increase in vigorous PA levels post-pandemic, only a small proportion of students achieved HEPA levels. The prevalence of walking as the primary form of PA, while beneficial, suggests that more efforts are needed to encourage higher-intensity activities. This highlights the importance of continued efforts to integrate PA into students' daily routines and provide access to facilities and programs that encourage regular, health-promoting PA.
Notably, our study did not find a statistically significant relationship between PA and stress levels among male students, contrasting with findings from other populations where PA was more strongly correlated with reduced stress in males. This discrepancy suggests the need for further research to understand the gender-specific effects of PA on stress.
Cluster analysis showed that higher PA levels co-occurred with lower perceived stress levels, while lower PA correlated with higher stress, findings which align with existing research. Additionally, Clusters 3 and 4, which showed unusual stress-PA patterns, had high LS scores, which may reflect socially desirable responding.
Our study underscores the need for tailored educational interventions and programs that address gender-specific needs in PA and stress management, particularly in the post-pandemic period. Enhancing awareness of the importance of adequate PA intensity and providing supportive environments for regular exercise may contribute to improving the well-being of medical students. Future research should aim to include more diverse and extensive participant pools to enhance the generalizability and depth of these findings.